Niger J Paed 2016; 43 (1): 20 – 25
ORIGINAL
Ajulo MO
Ocularhaemodynamics parameters of
Omole MK
asymptomatic HAART experienced
Moody JO
Olusanya BA
HIV-infected under-five children
DOI:http://dx.doi.org/10.4314/njp.v43i1.4
Accepted: 3rd August 2015
Abstract :
Objectives:
Study
experienced HIV-infected children
aimed at evaluating the impacts of
was 12.2cm/s while that of sero-
Ajulo MO
(
)
HAART on retinal blood flow of
negative children was 13.4 cm/s.
Department of Clinical Pharmacy and
a
s y m p t o m a t i c
H
A A R T -
The PI and RI of blood flow in
Biopharmacy,
University of Uyo,
experienced HIV-infected under-
CRA of asymptomatic HAART-
Uyo. Akwa-Ibom State.
five children.
experienced HIV-infected children
Nigeria.
Method: Ethical
approval and
were 0.8 and 0.5 respectively
Email: ajugbeng@gmail.com
patient consents were obtained
while those of the seronegative
before commencement of the
children were 0.6 and 0.4 respec-
Omole MK
study in the selected hospitals.
tively. Reduced Vmax of blood
Department of Clinical Pharmacy and
Thirty asymptomatic HAART-
flow of CRA was significantly
Pharmacy Administration,
experienced HIV-infected chil-
associated with both increased PI
Faculty of Pharmacy
dren and three seronegative chil-
and RI of asymptomatic HAART-
University of Ibadan,
Ibadan. Oyo State. Nigeria.
dren aged 0-5 year-old fulfilled
experienced HIV-infected under-
conditions for ocular ultrasono-
five children.
Moody JO
graphy among 60 convenience-
Discussion: Vmax
of CRA
of as-
Department of Pharmacognosy,
sampled under-fives. Ocular ultra-
ymptomatic HAART-experienced
University of Ibadan,
sonography was done on the pa-
HIV-infected children was reduced
Ibadan. Oyo State. Nigeria.
tients in supine position with eyes
because of their increased PI and
closed as instructed by the radi-
RI
suggesting an increased resis-
Olusanya BA
ologist.
Maximum
velocity
tance to blood flow in asympto-
Department of Ophthalmology,
(Vmax), pulsatility index (PI),
matic HAART-experienced HIV-
College of Medicine,
University of Ibadan,
resistive index (RI), optic nerve
infected children.
University College Hospital,
diameter, lens thickness and axial
Conclusion: Reduced
Vmax of
Ibadan. Oyo State. Nigeria.
diameter were measured. Results
blood flow to CRA was signifi-
of
HAART-experienced children
cantly associated with increased PI
were not compared with the con-
and RI of asymptomatic HAART-
trol children because of unequal
experienced HIV-infected chil-
size. Data were analysed by using
dren.
ANOVA and level of significance
was considered at p<0.05.
Keywords :
Ophthalmic artery,
Results: Vmax
of blood
flow in
Central retina artery, Maximum
central retinal artery (CRA) of
velocity, Seropositive children,
a
s y m p t o m a t i c
H
A A R T -
HAART
Introduction
sub-Saharan Africa are women. HIV-infection rates
among pregnant women in Africa range from 1% in
HIV/AIDS is a leading cause of childhood mortality and
Senegal to 40% in Botswana. In 2006, World Health
morbidity in Africa. In under-five children, HIV /AIDS
Organization (WHO) proposed that 2.3 million children
now accounts for 7.7% of mortality worldwide. AIDS
were living with Human Immunodeficiency Virus (HIV)
already accounts for a 36% rise in under- five’s mortal-
infection
mostly acquired through mother to child trans-
mission,
about 90% of them live in sub-Saharan Africa .
1
ity. In a state of declining immunisation, HIV/AIDS
threatens recent gains in infant and child survival and
health. The increased paediatric HIV infection rate in
1
AIDS affects children in many ways in Africa, about
Africa resulted from both increased HIV infection rate
400,000 children below 15 years died of AIDS in 2003.
in
childbearing women and the competence of Mother to
Demographic data from sub-Saharan Africa showed the
Child transmission (MTCT). Forty million persons were
impact of HIV on childhood mortality. Maternal ill
living with HIV in 2003, 70% of them lived in sub-
health such as HIV infection has a negative effect on
Saharan Africa while 60% of HIV-infected persons in
infant survival. Infant and early childhood mortality

21
among seronegative children of HIV-infected mothers is
study were children who were already above five years
2
to 5 times higher than that among seronegative chil-
and HIV-infected children who were not asymptomatic.
dren of HIV-negative mothers.
1
Recruitment of participants:
Forty (40)
HAART-
It
is assumed that over 1500 children are infected with
experienced HIV-infected children and 20 seronegative
HIV every day all over the world. HIV is responsible for
children were enrolled for the study. Thirty (30)
6%
of deaths in under-five children in Sub – Saharan Af-
HAART-experienced
HIV-infected children met the
rica. Recent data indicate that 40,000 HIV positive Afri-
criteria for ultrasonography while 3 seronegative chil-
can children received highly active antiretroviral therapy
dren met the criteria. The children who failed to meet
(HAART) in 2005. Nigeria has the highest burden of
criteria for ocular ultrasonography were due to their age
Mother- to- Child Transmission rates and Paediatric
which was slightly below four years and inability to stop
HIV disease in the world. Report on the Global AIDS
blinking the eyes during procedure. The participants
Epidemic showed that there are an estimated 240,000
were purposefully not sedated for the study.
HIV-infected children below 15 years old representing
Data collection: Data
were obtained
from successful
14% of the total African burden. In 2005, the Federal
2
ocular procedures on 30 HAART-experienced under-
Ministry of Health conducted biennial antenatal clinic
five HIV-infected children and 3 under-five seronega-
sentinel surveys, which showed HIV prevalence of 4.4%
tive children. As a result of unequal size, the result of
and 4.6% in 2007.
3
HAART-experienced HIV-infected children could not
be
compared with the seronegative children. Hence, the
The eye had been shown to be an important indicator of
association of hemodynamic parameters such Vmax, PI
the effects of teratogenic compounds, such as thalido-
and RI of the asymptomatic HAART-experienced HIV-
mide. Alcohol caused fetal alcohol syndrome which
4
infected children was determined.
was linked to structural abnormalities of the eye such as
microphthalmos, buphthalmos, coloboma, optic nerve
Ocular Ultrasonography
hypoplasia and increased tortuosity of the retinal ves-
sels.
5,6
This investigation was done for the detection of effects
of
HAART on retinal blood flow of seropositive chil-
The WHO commissioned systematic reviews on antiret-
dren. This investigation was performed only on thirty
roviral drug toxicities and laboratory monitoring strate-
asymptomatic seropositive children who had received
gies which include monitoring of potential increased
HAART for more than a year and three seronegative
risk of toxicity associated with the long-term use of anti-
children who were not on drugs. These children fulfilled
retroviral medicines in pregnancy, breastfeeding moth-
criteria for ocular ultrasonography procedures. Maxi-
ers andtheir children. It is important to monitor the use
mum velocity (Vmax), pulsatility index (PI) and resis-
of
antiretroviral drugs in poor economy countries where
tive index (RI) of blood flow in central retinal artery and
toxicities may present a different pattern in association
ophthalmic artery were examined. Optic nerve diameter,
with either environmental or behavioural factors.
7
axial diameter and lens thickness of the eyes were also
This study aimed at evaluating the impacts of HAART
examined. Medical personnel in radiology unit of the
on
retinal blood flow of 0-5 year-old asymptomatic HIV
University College Hospital had software on ultrasono-
-infected children on HAART in Southern Nigeria.
graphy equipment which could only perform assessment
of
Vmax, PI, RI and optic nerve diameter while those in
University of Uyo Teaching Hospital could only do as-
sessment of axial diameter and lens thickness. In this
Method
respect, data from the two centers were analysed sepa-
rately. Due to failure of majority of the study control
Study design: In
order to
observe effects
of HAART
on
participants to meet the criteria for ocular ultrasonogra-
heamodynamic parameters of the eyes of asymptomatic
phy such as keeping the eyes closed during procedure
HAART-experienced HIV-infected under-five children,
and absence of primary standard parameters in Nigeria
a
quantitative, observational approach was used.
and Africa, standard parameters from similar study in
Study setting: Forty
(40) HIV-infected
children aged
0-
USA and Sweden were adopted.
5
years old, who had been on HAART for more than a
year and 20 seronegative children were recruited for the
Ocular ultrasonography procedure
study in University College Hospital, Ibadan and Uni-
versity of Uyo Teaching Hospital. Consent of care-
The ultrasonography scans were performed with the
givers of participants was obtained after ethical approval
patient in supine position, eyes closed and directing gaze
was received from the study centers.
towards the ceiling. Ultrasound scanners and 5-10MHz
Study population: Convenience sampling
was used
to
linear array transducers were used. Transducers were
enrol 60 participants aged 0-5 years old who attended
applied with contact jelly through the closed upper eye-
either HIV clinic or the general outpatient department.
lid while the examiner’s hand rested upon the orbital
Inclusion criteria: Selection of
participations for
the
margin to minimize the pressure on the globe. Blood
study was based on age 0-5 years, both male and female,
flow in the retrobulbar orbit was detected by the produc-
asymptomatic HIV-infected children in WHO Stage 1
tion of colour pixel on the visual display unit. The mini-
and seronegative children from seronegative mothers.
mum size of sample gate used was 1.2mm X 1.2mm
Exclusion criteria: Those
who were
not included
in the
with the Siemens machine. It was directed to a blood
22
vessel. The spectra analysis of the resultant frequency
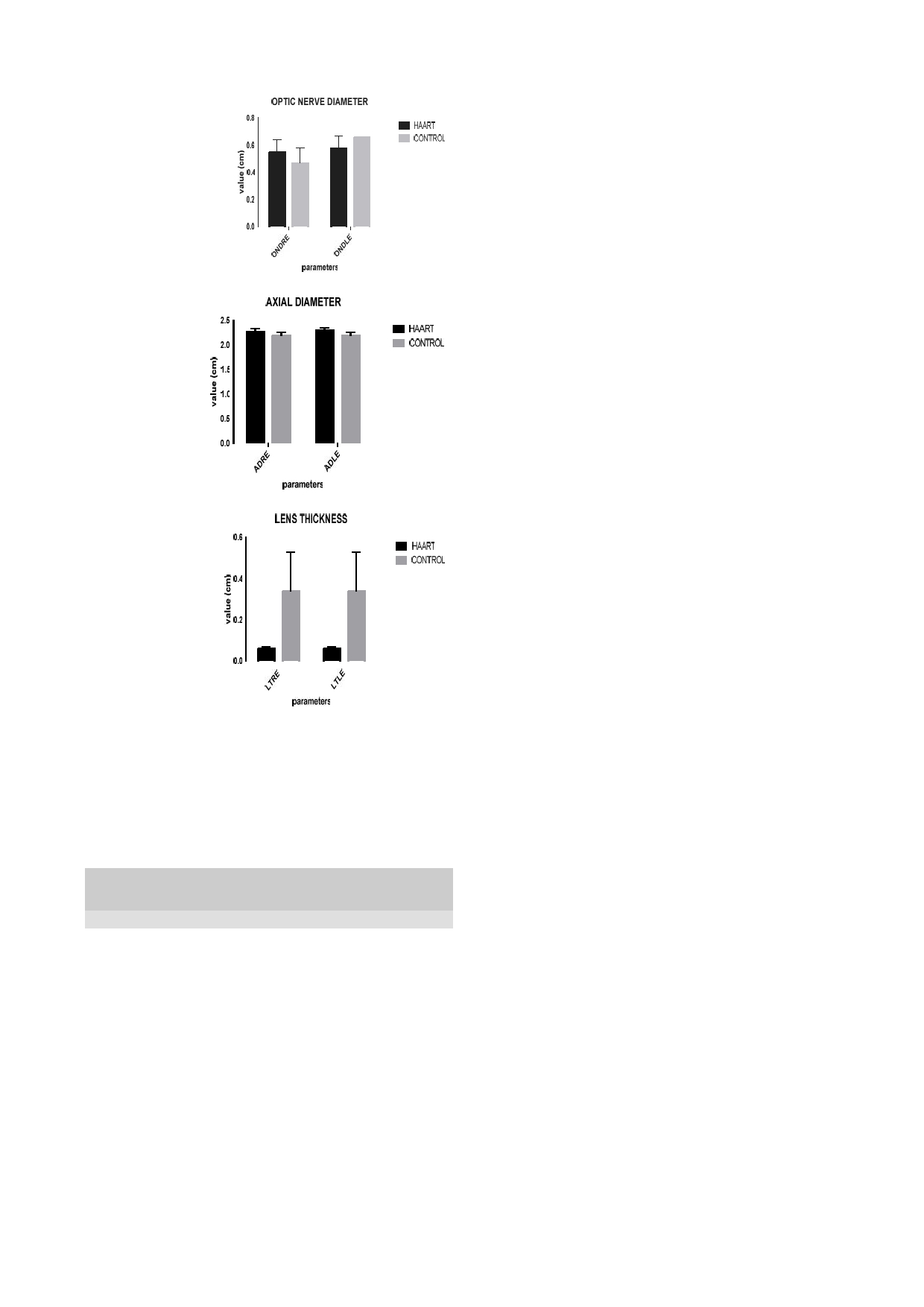
tic nerve diameter of the right eye of asymptomatic sero-
shift was used to obtain a velocity waveform. The wave-
positive children on HAART was 0.5 cm while that of
form consisted of multiple velocities, the peak velocity
seronegative children was 0.4 cm (Fig. 3), (Table 2).
values were used in the analyses. In artery, the peak sys-
The ocular ultrasonography measurements of asympto-
tolic velocity (PSV) and end diastolic velocity (EDV)
matic seropositive children on HAART in UUTH
were used. Since these measures provided no informa-
showed that the mean of axial diameter of right eye was
tion of the waveform, two indices were used:
2.2 cm while that of the left eye was 2.3 cm (Fig. 4).
Resistive index (Pourcelot’s ratio) = PSV-EDV
Lens thickness of right eye of seropositive children on
PSV.
8
HAART was 0.1 cm (Fig. 5) and that of the left eye was
Pulsatility index =
PSV-EDV
0.1 cm (Table 2).
Tmax.
9
NB:
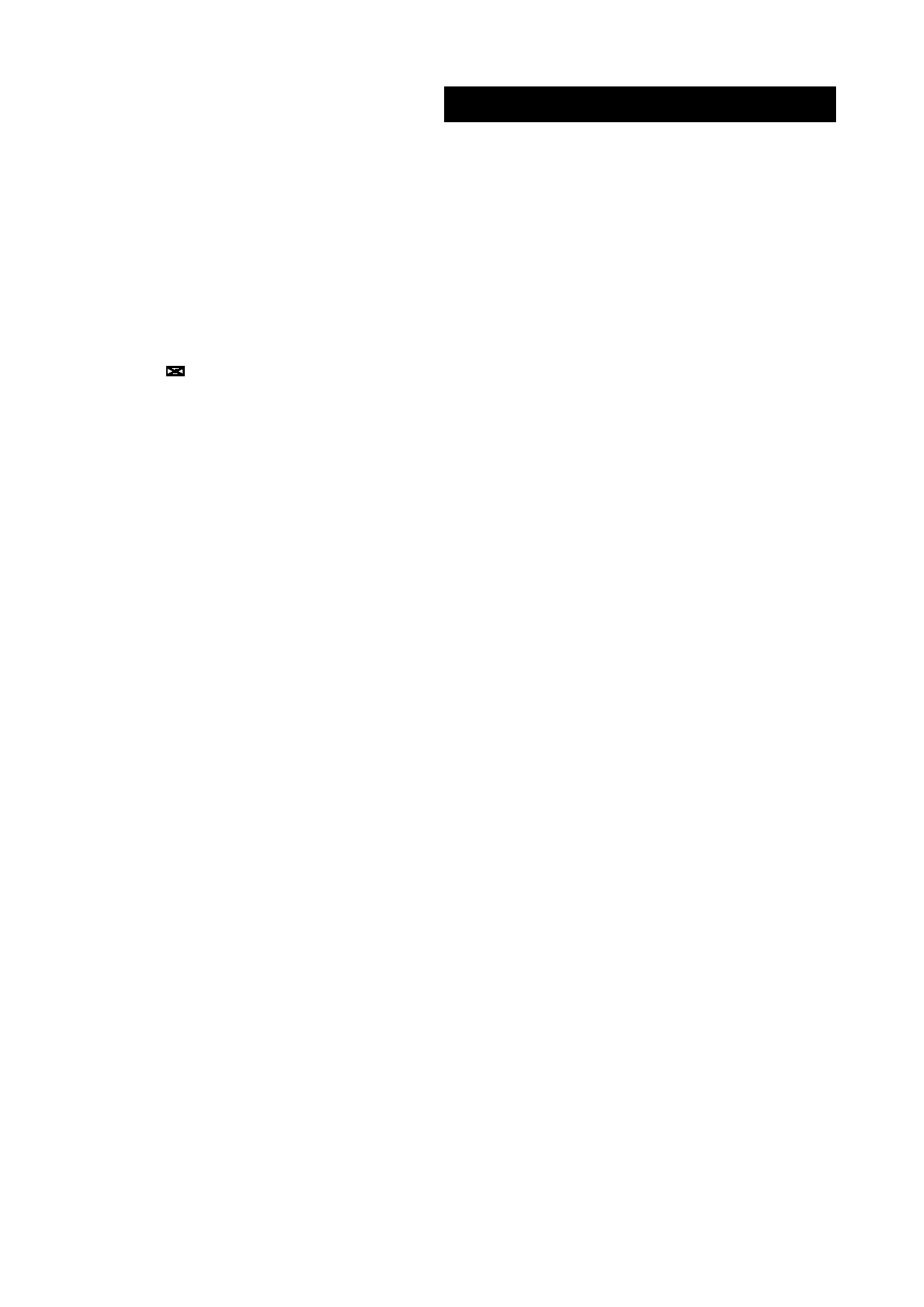
Fig 1: Comparison
of blood
flow in
central retinal
artery of
Tmax: Is
the time
averaged peak
velocity
children on HAART and seronegative children (control)
Resistive index is usually quoted from 0-100% (0-1)
with 0 representing no resistance and 100 representing
high resistance.
Data management and analysis:
Data was
stored using
Microsoft Office 2008. Data was analysed by using de-
scriptive statistics and analysis of variance (ANOVA).
Statistical significance was considered at level p < 0.05.
Statistical Package for the Social Sciences (SPSS) soft-
ware version 20.0 (SPSS Inc. Chicago, III, USA) was
used for the analysis.
Results
Ocular ultrasonography measurement
The mean age of study participants was 4.71±0.59 years,
Table 2: Ocular
ultrasonography
measurement
15
(45.45%) boys and 18 (54.55%) girls successfully
S/n
Region
Eye
Pars
Mean
Control
performed ocular ultrasonography (Table 1).
Children on
(cm)
HAART (cm)
Table 1: Demographic
characteristics of
participants
UC
Central
Right
Vmax
12.2±3.6
13.4±1.5
1
H
retinal
PI
0.8±0.3
0.6±0.1
s/n
Character
Frequency
Artery
RI
0.5±0.1
0.4±0.0
i
Age
(years)
4.71±0.59
Left
Vmax
13.2±4.5
13.1±0.0
ii
Male
15
(45.45%)
PI
0.8±0.3
0.7±0.0
iii
Female
18
(54.55%)
RI
0.5±0.1
0.3±0.0
Total
33
Oph-
Right
Vmax
23.6±9.1
33.8±4.0
thalmic
PI
1.4±0.4
0.8±0.5
The
ocular ultrasonography measurements of asympto-
artery
RI
0.7±0.1
0.4±0.2
Left
Vmax
24.0±8.1
42.1±0.0
matic seropositive children on HAART in UCH showed
PI
1.5±0.4
1.5±0.0
that the mean of maximum velocity (Vmax) of blood
RI
0.7±0.0
0.7±0.0
flow in Central retinal artery (CRA) of eyewas12.2 cm/s
Optic
Right
Diameter
0.5±0.1
0.4±0.1
while that of seronegative children was 13.4 cm/s
nerve
Left
Diameter
0.5±0.1
0.6±0.0
1
2
UU
axis
Right
Diameter
2.2±0.0
2.2±0.1
(Fig. 1). The pulsatility index (PI) of blood flow in CRA
1
TH
Left
Diameter
2.3±0.0
2.2±0.1
of
eye of asymptomatic HIV-infected children on
2
Lens
Right
Thickness
0.1±0.0
0.3±0.1
0.30.1
2
HAART was 0.8while that of the seronegative children
Left
Thickness
0.1±0.0
was 0.6. The Resistive index (RI) of blood flow in CRA
Obtained from Swedish study.
14,15
of
eyeof asymptomatic HIV-infected children on
Obtained from United States study.
18
HAART was 0.5while that of the seronegative children
Vmax- maximum velocity, PI- pulsatility index, RI- resistive index
was 0.4 (Table 2).
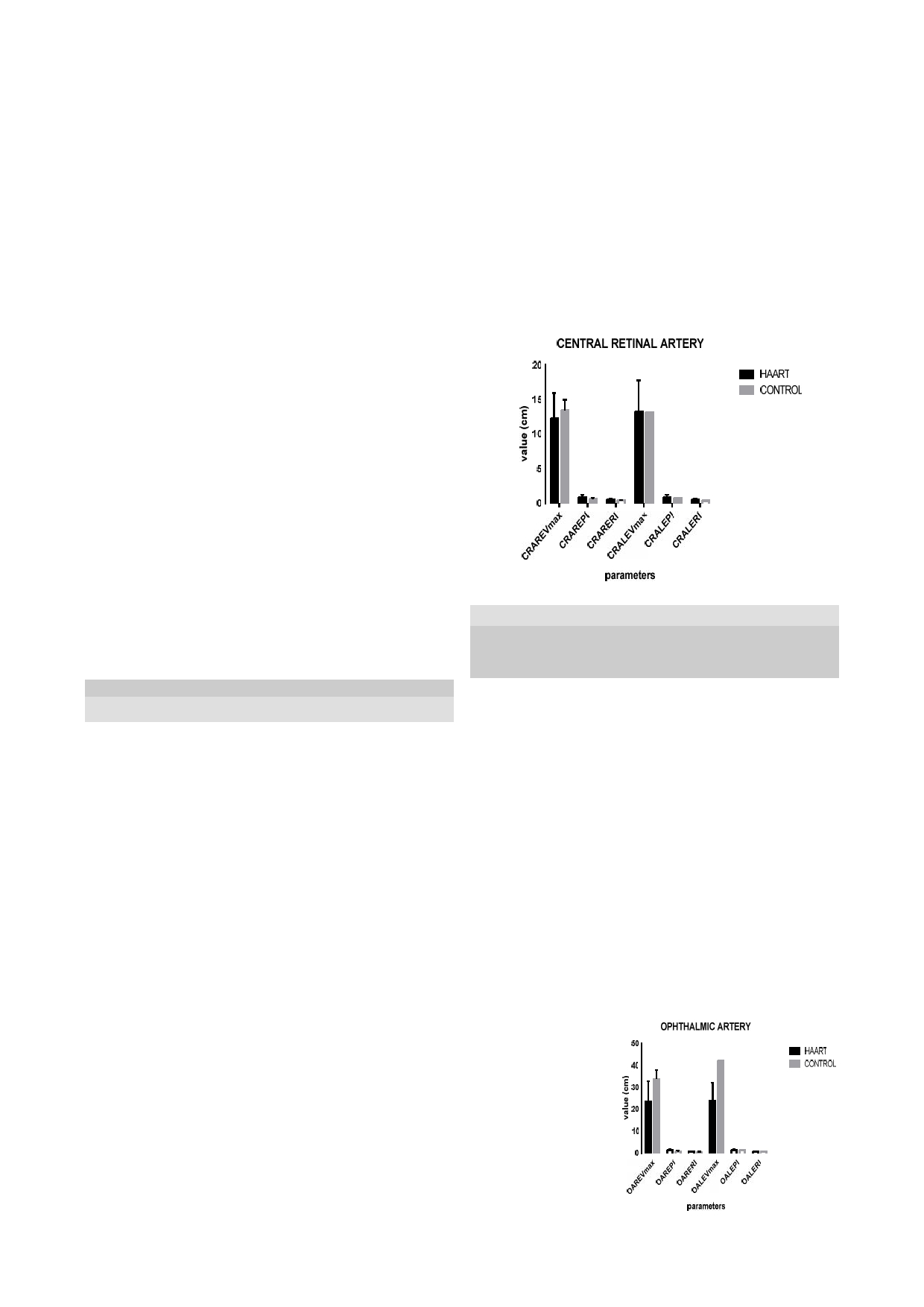
The Vmax of blood flow in ophthalmic artery of eye of
Fig 2: Comparison
of
asymptomatic seropositive children on HAART was
blood flow in ophthal-
23.6 cm/s while that of the seronegative children was
mic
artery of children
on
HAART and sero-
33.8 cm/s (Fig. 2). PI of blood flow in ophthalmic artery
negative children
of
eye of asymptomatic HIV-infected children on
(control)
HAART was 1.4 while that of seronegative children was
0.8. RI of blood flow in ophthalmic artery of eye of as-
ymptomatic seropositive children on HAART was0.7
while that of the seronegative children was 0.4. The op-
23
Discussion
Fig 3: Comparison
of
optic nerve diameter
Maximum velocity of central retina artery (CRA) of the
between children on
eye of seropositive children on HAART was reduced
HAART and seronega-
because of their increased pulsatility index (PI) and re-
tive (control) children
sistive index (RI). This possibly suggested that increased
pulsatility index indicated an increased resistance to
ocular blood flow in children receiving HAART. This
finding in asymptomatic HAART-experienced HIV-
infected under-fives supports the claims of previous
studies.
9,10
Williamson had documented in their study
Fig 4: Compari-
that reduced velocity was detected in the central retinal
son
of axial di-
artery of patients with progressive non-arteritic ischemic
ameter of children
optic neuropathy when compared with unaffected con-
on
HAART and
tralateral eyes. The central retinal artery velocity was
control children
increased while the pulsatility index in the posterior
ciliary arteries was reduced after optic nerve sheath de-
compression following an immediate postoperative pe-
riod. Observation of patients with chronic papilledema
from pseudotumor cerebri indicated reduced velocities
in
the central retinal and posterior ciliary arteries with an
increased pulsatility index in the central retinal artery
when compared to controls. Following optic nerve
sheath decompression after 48 hours, an increase in the
blood velocities was observed in patients with improved
Fig 5: Comparison
vision which was due to increased perfusion of the
of
lens thickness of
blood vessels.
9
children on HAART
and
control children
Maximum velocity of ophthalmic artery (OA) of the eye
of
asymptomatic seropositive children on HAART was
reduced because of their increased PI and RI. The in-
creased PI and RI possibly suggested an increased resis-
tance to blood flow. This finding in asymptomatic
HAART-experienced HIV-infected under-fives supports
claim of previous study.
9,10
Williamson in their study
affirmed that both pulsatility and resistive indices pro-
Maximum velocity (Vmax) of blood flow of both central
vide an indication of the effects of resistance on blood
retinal artery and ophthalmic artery was compared with
flow in the retinal blood vessels.
9
both pulsatility index (PI) and resistive index (RI) in
Increased optic nerve diameter of the eye was observed
eyes of asymptomatic seropositive children on HAART.
among asymptomatic seropositive children on HAART
Axial diameter was compared with lens thickness in
regimens which may suggest effect of HAART. Earlier
eyes of asymptomatic seropositive children on HAART.
study showed that increased optic nerve diameter was
The results were significant (Table 3).
associated with elevated cerebrospinal fluid pressure and
intracranial pressure.
11,12,13
Ballantyne in their study ex-
Table 3: Comparison
of ocular
parameters of
children on
HAART
plained that the optic nerve diameter in children below 1
year is indicated to have normal values from 0.21-
Ocular parameters
p-value
0.40cm and for children above 1 year of age is 0.24-
Central
Right
Vmax
PI
P<0.001
0.43cm. The normal range of values for children of age
retina ar-
eye
RI
P<0.001
1-15 years is close to the normal values of optic nerve
tery
Left eye
Vmax
PI
P<0.001
diameter in adult. An optic nerve diameter greater than
RI
P<0.001
0.4cm in infants less than 1 year of age, while 0.45 cm
Ophthalmic
Right
Vmax
PI
P<0.001
or
greater in older children are considered as abnormal.
artery
eye
RI
P<0.001
Increasedoptic nerve sheath diameter was indicated in
Left eye
Vmax
PI
P<0.001
RI
P<0.001
patients suffering from intracranial hypertension which
Axial di-
Right
Axial
Lens
P<0.001
returned to normal values after surgical or medical treat-
ameter
eye
diameter
thickness
ment. An increased optic nerve diameter was also indi-
Left eye
Axial
Lens
P<0.001
cated in elevated cerebrospinal fluid pressure and intrac-
ranial pressure. However, there is a need to determine
11
diameter
thickness
Vmax- maximum velocity, PI- pulsatility index, RI- resistive index
normal values of ocular hemodynamic parameters for
under-fives in Nigeria.
In
absence of control group and lack of normal data,
24
axial diameter of the eye of asymptomatic seropositive
diameter of the eyes of asymptomatic seropositive chil-
children on HAART was compared with a Swedish nor-
dren who were on HAART.
mal value for age 3-5 years (2.07-2.34 cm). Comparing
the mean, it could be suggested that the axial diameter of
children on HAART was normal.
14,15
Conclusion
In
spite of all the differences in ocular parameters be-
tween the asymptomatic seropositive children on
This study has shown significant association between
HAART and control children, there was no physical
reduced maximum velocity of blood flow in both oph-
observation of abnormality in the vision of the asympto-
thalmic artery and central retinal artery with increased
matic seropositive children on HAART. This observa-
pulsatility and resistive indices of the eyes of asympto-
tion was in support of findings obtained by Ogunbosi et
matic seropositive children on HAART. Similarly, lens
al., in their study on clinical pattern of HIV-infection
thickness was significantly linked to the axial diameter
among children at the same site of this study. In their
of
the eyes of 0-5year old asymptomatic seropositive
study, there was no indication of cytomegalovirus infec-
children on HAART.
tion and any other ocular diseases among clinical pattern
of
HIV infection illustrated in children with advanced
Recommendation
stage of AIDS .Similar observation was made by Fetuga
3
et
al in their ten year review of paediatric HIV/AIDS
Vision test should be incorporated in the monitoring of
among hospitalized children in another study site in
adverse events in under-five children on HAART. More
Southwest Nigeria. This obviously rules out involve-
16
studies involving a large number of HIV-infected chil-
ment of HIV infection in reduced blood velocity of oph-
dren on HAART should be done to evaluate impacts on
thalmic artery and central retinal artery. Yung et al.,
ocular hemodynamic parameters.
observed that adult HIV positive patients with AIDS
showed a statistically significant reduction of perifoveal
capillary blood flow velocity in a study performed in
Authors’ contribution
United States of America. In this study, asymptomatic
17
AMO designed the study, performed field work, wrote
HAART-experienced HIV-infected under-five children
manuscript, OMK and MJO participated in designing
were involved. Therefore, HIV infection appears not to
the study, supervised work and edited the manuscript;
have been the cause of reduced blood velocity in both
OBA took care of technical aspect of the study and ed-
ophthalmic and central retinal arteries. However, the
ited the manuscript.
observed differences could have serious implication in
Conflict of interest: None
the future of these children.
Funding : None
The association of reduced maximum velocity (Vmax)
with pulsatility index (PI) and resistive index (RI) of
both central retinal artery and ophthalmic artery of the
Acknowledgement
eyes of asymptomatic seropositive children on HAART
were statistically significant. Similarly, there was sig-
The supports of staff of radiology department and HIV
nificant association between lens thickness and axial
centres were appreciated.
References
1.
Tindyebwa D, Kayita J, Musoke
4.
Stromland K and Miller MT. Re-
8.
Constantino R., Patrizia P, Enrico
P ,
Eley B, Nduati
R, Coovadia H,
fractive evaluation of thalidomide
Z,
Carmen G, Maria C and
Bobart R, Mbori- Ngacha D and Kief-
embryopathy .
Graef Arch
Clin Exp
Giuseppe T. Normal neonatal val-
fer
MP. Handbook on Pædiatric AIDS
Ophthalmol 1992; 230: 140- 149.
ues
of ophthalmic and central reti-
in
Africa by the African Network for the
5.
Stromland K. Ocular abnormalities
Care of Children Affected by AIDS. 2006
nal
artery blood flow velocities. J.
in
the fetal alcohol syndrome. Acta
available at www. anecca. org and
Peadiat Ophthalmology Strabis-
www.rcqhc.org, retrieved on
23/06/2015.
Ophthalmol (Copenh) 1985; 63:
mus 2001; 38(4): 213-217 .
2.
Federal Ministry of Health. Na-
(Suppl 171).
9.
Williamson TH and Harris A. Col-
tional guidelines for paediatric
6.
Hellstrom A, Jansson C, Bo-
our
doppler ultrasound imaging of
HIV
and AIDS treatment and care.
guszewski M, Olegird M, Laegreid
the
eye and orbit. Survey
Ophthal-
2007. Retrieved on 23/06/2015.
L
and Albertsson- Wikland K.
mology 1996; 40(4): 255-267.
3.
Ogunbosi BO, Oladokun RE,
Growth hormone status in six chil-
10.
Baxter GM, Williamson TH,
Brown BJ and Osinusi KI (2011).
dren with fetal alcohol syndrome
.
Mckillop G and Dutton GN. Col-
Prevalence and clinical pattern of
Acta Pediatr 1996; 85: 1456-
our
Doppler
ultrasound of orbital
paediatric HIV infection at the Univer-
1462.
and
optic nerve blood flow: Effects
sity College Hospital, Ibadan, Nigeria:
7.
World Health Organisation. Con-
of
posture and timolol 0.5%. Inves-
a
prospective cross-sectional study.
solidated guidelines on the use of
Italian Journal of Pediatrics 2011; 37(29): 1-
tigative Ophthalmol Visual Science
antiretroviral drugs for treating and
6
http://www.ijponline.net/content/37/1/29.
1992; 33: 604-610.
retrieved on 23/06/2015.
preventing HIV-Infection. Recom-
mendations for a public health
approach. 2013. www.who.int

25
11.
Ballantyne J, Hollman AS, Hamil-
14. Hellstrom
A, Svensson
E, Strom-
17.
Yung C-W, Harris A, Massicotte
ton
R et al.Transorbital optic nerve
land K. Eye size in healthy Swed-
S,
Chioran G, Krombach G, Danis
shealth ultrasonography in normal
ish
children and in children with
R
and Wolf S. Retinal blood flow
children. Clinical
Radiology 1999;
fetal alcohol syndrome. Acta Oph-
indices in patients infected with
54: 740-742.
thalmologica Scandinavica 1997;
human immunodeficiency virus.
12.
Galetta S, Byrne SF and Smith JL.
75:423-428.
British J. Ophthalmology 1996;
Echographic correlation of optic
15.
Youn DH, Yu YS and Park IW.
80: 723-727.
nerve shealth size and cerebrospi-
Intraocular pressure and axial
18.
Lehman BM, Bernstein DA, Bailey
nal
fluid pressure. J.
Clinical
length in children. Korean
J Oph-
MD
and Zadnik K. Validation of
Neuro-ophthalmology 1989; 9:79-
thalmology 1990; 4: 26-29.
OCT
– based crystalline lens thick-
82.
16.
Fetuga MB, Ogunfowora OB,
ness measurements in children.
13.
Cennamo G, Gangemi M and
Oyegunle VN and Thanni LOA. A
Optometry Vision Science 2009; 86
Stella L. The correlation between
ten
year review of paediatric HIV/
(3): 181-197.
endocrinal pressure and optic
AIDS among hospitalized children
nerve diameter: an ultrasonogra-
in
a Nigerian teaching hospital.
phy
study. In: Ossoinig KC. Ed.
Niger J. Paediat 2005; 32 (3): 29-
Ophthalmic echography 1987; 603
32.
-606.